Tracheoesophageal
Introduction
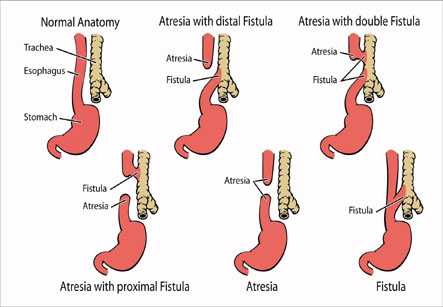
Tracheoesophageal fistula is a disorder involving an abnormal connection at one or more places between the esophagus (the food-pipe) and the trachea (the tube that leads from the throat to the windpipe and lungs). Normally, the esophagus and the trachea are two separate tubes which are not connected.
Tracheoesophageal fistula is also known as TE fistula or simply TEF.
TE fistula is a birth defect, which is an abnormality seen in the fetus as it is forming in the mother’s uterus.
When a baby with a TE fistula swallows, the liquid can pass through the abnormal connection between the esophagus and the trachea. As a result, the liquid can get into the baby’s lungs. This can cause aspiration pneumonia and other problems.
Iranian specialists have made remarkable achievements in infants' surgeries and Iran is among few countries that have gained access to the latest surgical technologies
Causes of tracheoesophageal fistula:
As a fetus is growing and developing in the mother’s womb before birth, different organ systems are developing and maturing. The trachea and the esophagus usually begin developing as one single tube. At about four to eight weeks after conception, a wall forms between the esophagus and trachea to separate them into two distinct tubes. If this wall does not form properly, TE fistula and/or esophageal atresia can occur.
Incidence
Tracheo-esophageal fistula is often associated with other birth defects in the baby, such as:
1. Trisomy 13, 18, or 21
2. Other digestive tract problems such as diaphragmatic hernia, duodenal atresia, or imperforate anus
3. Heart problems such as tetralogy of Fallot, ventricular septal defect, or patent ductusarteriosus
4. Kidney and urinary tract problems which may be horseshoe or polycystic kidney, absent kidney, or hypospadias
5. Muscular or skeletal problems
6. VACTERL syndrome which involves Vertebral, Anal, Cardiac, TE fistula, Renal, and Limb abnormalities
Up to one-half of all babies with TE fistula have another birth defect.
Symptoms of TE fistula
The symptoms of TE fistula are usually noted very soon after the birth. The following are the most common symptoms of TE fistula. However, the symptoms experienced by each child may vary. Symptoms may include the following:
1. Frothy white bubbles in the mouth
2. Coughing or choking during attempts at feeding
3. Vomiting
4. Blue discoloration of the skin (cyanosis), especially when the baby is feeding
5. Difficulty in breathing
6. Very round, full abdomen
Diagnosis:
A complete physical examination is done and medical history is elicited. Imaging studies are usually done to evaluate whether a baby has TE fistula. X-rays are taken to look at the chest and abdomen of the baby.
A small tube may also be placed into the mouth or nose and then guided into the esophagus. If the child has esophageal atresia, the tube usually cannot be inserted very far into the esophagus. The tube’s position in the esophagus can also be seen with the x-ray.
Treatment for TE fistula:
If the baby has TE fistula, he/she will need surgery immediately to fix the problem. The type of surgery depends on the following:
1. Type of abnormality present
2. General health of the baby and medical history
3. Opinion of the surgeon and other physicians involved in the baby’s care
4. Expected course of the condition
5. Opinion and preference of parents
TE fistula is a birth defect, which is an abnormality seen in the fetus as it is forming in the mother’s uterus.
During the repair of TE fistula, the connection between the esophagus and the trachea is closed in surgery. In associated esophageal atresia, the repair depends upon how close the two sections of esophagus are to each other. Sometimes esophageal atresia requires more than one surgery. The baby’s surgeon and other physicians will decide the best time for the operations, based on the type of the problem and the baby’s condition.
Problems in the future:
Some children born with TEF or esophageal atresia may have long-term problems.
1. Swallowing food or liquids may be difficult due to:
2. Problems with the normal rhythmic movement of foods and liquids down the esophagus (peristalsis).
3. Scarring of esophagus occurring after surgery as the wounds heal. This can partially block the passage of foods.
Sometimes, a narrowed esophagus can be widened or dilated with a special procedure done under general anesthesia. In other cases, another operation may be necessary to open up the esophagus for the proper passage of the food to the stomach.