Gastroschisis
Introduction
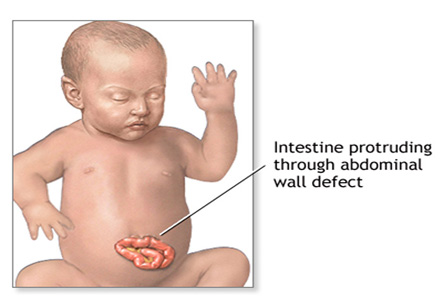
Gastroschisis is a congenital condition in which there is incomplete formation of the abdominal wall so that the contents protrude outside the body. There is no membrane (peritoneum) covering over the abdominal contents. The opening is usually located to the right of the umbilicus. Typically the opening is very small, but it can sometimes be very large in size. The amount and type of protruding abdominal contents may vary, but it is commonly intestinal tissue. The bowel tissue floats in the amniotic fluid before birth, and this contact with amniotic fluid may damage the bowel tissue, which can affect its appearance and function.
Sometimes gastroschisis can be detected in early in pregnancy on a fetal ultrasound or by an elevated maternal or amniotic serum alpha-fetoprotein level. The baby may be sometimes delivered early (at 35 weeks instead of at 40 weeks, which is full-term) to limit the extent of damage to the bowel tissue.
Incidence:
Gastroschisis occurs in 2 out of 10,000 live births. Boys are affected more than girls by this condition. It is very rare for this condition to recur in subsequent pregnancies.
Iranian specialists have made remarkable achievements in infants' surgeries and Iran is among few countries that have gained access to the latest surgical technologies
Common associated problems:
Most cases of gastroschisis are associated with:
1. Prematurity
2. Intrauterine growth retardation (below-average growth before birth)
3. Cardiac problems
4. Shortened bowel length
5. Maternal illness and infection
6. Genetic abnormalities
7. Other intestinal abnormalities such as intestinal atresia
Treatment and outcomes:
Babies with gastroschisis are best treated in a specialized pediatric hospital having experience in treating children with complex conditions. Surgery is performed as soon as the baby is stable after delivery to prevent infection or damage to intestinal tissues. A tube is inserted through the baby’s nose or mouth prior to surgery to remove all fluids from the gastrointestinal tract using suction. A course of antibiotics is given to combat infection.
A hernia of the abdominal wall can occur in later childhood or adulthood, which may require additional surgery to repair.
If the opening is small (in about 80% of the cases), the bowel contents are carefully placed into the abdomen if the tissue appears healthy. After this, the hole will be surgically closed. However, sometimes this is not possible and a silicon patch is used to cover the exposed bowel. Babies are given total parenteral or intravenous nutrition until the bowel is healed. Once the bowel is functioning, oral feedings of breast milk or formula can be safely tolerated.
Improved surgical techniques and facilities of neonatal care have resulted in an 85-90% survival rate of babies with gastroschisis in recent years. However, babies with gastroschisis will require long hospitalizations, and complications are quite frequent.
Complications:
Babies born with gastroschisis are prone to hypothermia (low body temperature), dehydration (lack of body fluids), sepsis (infection throughout the body), and hypoglycemia (low sugar level in the blood) as a results of exposed bowels.
After surgery, parents have to watch the babies very closely for any signs of bowel obstruction, due to infection, scarring or twisting on itself (called volvulus). Babies with a bowel obstruction can vomit bile-colored fluid, be irritable and have a swollen abdomen.
A major complication of gastroschisis is short bowel syndrome which occurs due to damage or infection of a large section of the bowel. This bowel infection occurring after birth is called necrotizing enterocolitis (NEC), and it needs to be treated immediately when it is suspected. The child’s nutrition may be severely affected. Some children do have to be on life-time TPN because of short-bowel conditions.
A hernia of the abdominal wall can occur in later childhood or adulthood, which may require additional surgery to repair. Children may require periodic assessment from gastrointestinal specialists, nutritionists and surgeons.
Future implications on child’s development:
The effects on a child’s development can vary according to the extent of the condition and also the complications. If the baby is treated in infancy and if there is no short-bowel syndrome, the treatment is very successful (85% success rate). Prolonged illness, immobility, lack of good nutrition, and multiple surgeries may delay the baby’s development. However, once the initial crises phase passes, babies can often catch up with their development with early infant stimulation programs. The infants are prone to infection until the healing has occurred and good nutrition is established.
Surgical scars on the abdomen might be extensive and may cause self-consciousness, especially during adolescence. Children need to be supported by family and friends to understand their condition and be confident, independent individuals in life.