Esophageal Atresia
Introduction
Esophageal atresia is a structural anomaly of the digestive system in which the esophagus does not develop properly. The esophagus or food pipe is the tube situated in the chest that carries food from the mouth to the stomach.
Causes:
Esophageal atresia is a type of congenital defect, which means it occurs before birth of the child. There are several types of this condition. In the most common type, the upper esophagus ends in a blind pouch and does not connect with the lower part of esophagus and stomach. The top end of the lower esophagus connects to the windpipe or trachea. This connection between pathway for food and air is called a trachea-esophageal fistula or TEF. This anomaly can be associated with other problems like such as heart defect or other digestive tract disorders.
Iranian specialists have made remarkable achievements in infants' surgeries and Iran is among few countries that have gained access to the latest surgical technologies
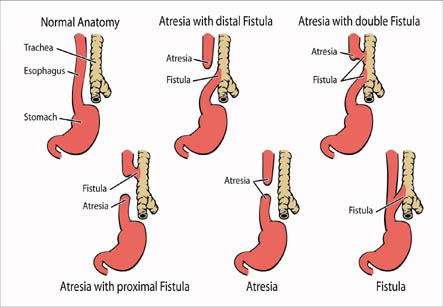
Other types of esophageal atresia:
• Both upper and lower segments of the esophagus end in pouches. No TEF.
• The lower segment ends in a blind pouch, TEF of the upper segment. This is rare.
• TEF in both upper and lower segments. This is extremely rare. This condition has possibility of occurring in one baby out of 4,000 births.
The other birth defects associated with esophageal atresia may be:
• Trisomy 13, 18 or 21
• Other digestive tract problems including diaphragmatic hernia, intestinal atresia or imperforate anus
• Heart defects such as ventricular septal defect, tetralogy of Fallot or patent ductusarteriosus
• Horseshoe or polycystic kidney, hypospadias
• Muscular or skeletal problems
• VACTERL syndrome- This is a non-random collection of abnormalities that can also involve defects of the spine, heart, lower digestive tract, kidneys and limbs. The combination of defects is variable.
Symptoms:
1. The child may show bluish coloration of the skin known as cyanosis when feedings are attempted.
2. Coughing, gagging, and choking with attempted feeding
3. Drooling of saliva
4. Poor feeding and failure to thrive
Diagnosis:
1. Before birth, an ultrasound can be performed on the pregnant mother showing excessive amount of amniotic fluid, which can be a predisposing condition for esophageal atresia or other structural problems of the digestive tract.
2. Clinically, the disorder can be diagnosed shortly after birth when feeding is attempted by the mother and the infant starts coughing, choking, and turning blue. As soon as the diagnosis of esophageal atresia is suspected, a procedure to pass a small feeding tube through the mouth or nose into the stomach is performed. If the feeding tube is not able to pass all the way to the stomach, the baby has esophageal atresia.
3. An x-ray of the chest and abdomen shows an air-filled pouch in the chest and air in the stomach and intestine. If a feeding tube has been inserted, it will appear in X-ray as a coiled up tube in the upper part of esophagus.
Treatment:
Esophageal atresia is considered as surgical emergency. This surgery to repair the esophagus should be performed as soon as possible after the baby is stabilized so that the lung damage is prevented and feeding can be continued. The surgery is usually done between 2 to 6 months of age.
This anomaly can be associated with other problems like such as heart defect or other digestive tract disorders.
In some children, the two ends of esophagus are so far apart that they cannot be easily connected. This is known as long-gap esophageal atresia. This is treated by esophageal lengthening procedures such as Foker process. This is a technique of stimulating the upper and lower ends of the esophagus to grow so they could be joined together. The time period required for this may vary depending on the gap between two ends of esophagus. However, the two ends can usually be attached together in about two to five weeks.
Before the surgery, the baby is not fed by mouth. Care is taken to prevent the baby from breathing secretions into the lungs.
Prognosis:
An early diagnosis of the condition provides better chances of having a good outcome. After proper treatment, most babies with esophageal atresia can start to eat normally within two to three months. The child needs to be monitored for strictures (places of narrowing) in the esophagus, but usually this is treatable.
Possible Complications:
• The most dangerous complication in the infant is breathing of saliva and other fluids into the lungs causing infection in the lung. This is called as aspiration pneumonia which may lead to choking, and possibly death.
• Feeding problems.
• Reflux or return of food from the stomach back into mouth.
• Narrowing of esophagus due to scarring from surgery.