Repair Fracture Radius
Introduction
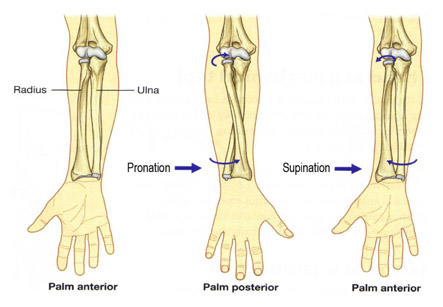
Radius and ulna are two bones of the forearm. They help to form wrist joint at one end and elbow joint at the other. The radius, ulna, and humerus articulate in such a way as to form four distinctive joints at the elbow. Surrounding the osseous structures are the ulnar collateral ligament, the lateral collateral ligament complex and the joint capsule. Four main muscle groups provide movement at the elbow joint, which include the flexors, extensors, pronators and supinators groups.
Different types of radial head fractures can occur. Each of these has separate surgical indications and considerations. Fractures of the proximal one-third of the radius normally occur in the head region in adults and in neck region in children.
While trying to break a fall by putting the hand out in front of you is an instinctive response. But the force of the fall can travel up the lower forearm bones and dislocate the elbow. It also can break the smaller bone (radius) in the forearm. A break can occur at the head of radius near the elbow.
Iran ranks among the top 10 countries in orthopedics and Iranian surgeons perform high quality orthopedic surgeries at highly affordable prices
Causes- Radial head fractures are common injuries which occur in about 20 percent of all acute elbow injuries. They are more frequent in women than in men and occur most often between ages of 30 and 40 years. In about 10 percent of all elbow dislocations, there is accompanying fracture of the radial head. As the upper arm bone (humerus) and the ulna return to their normal alignment, a piece of the radial head bone can be chipped off.
The most recognized and used standard for evaluating radial head fractures is the Mason classification system. It is used for both treatment and prognosis purpose.
1. Type I fracture- A marginal fracture without displacement.
2. Type II fracture- Marginal fractures with displacement involving greater than 2 mm displacement.
3. Type III fracture- Comminuted fractures of the radial head.
4. Type IV fracture (variation)-Comminuted fracture, with an associated dislocation, ligament injury, coronoid fracture, or Monteggia fracture.
Pathogenesis:
Severe comminuted fractures or fracture dislocations of the head of the radius often occur as the result of a fall on an outstretched arm with the distal forearm angled laterally. Fractures can also occur from a direct blow on the elbow (e.g. MVA). Damage of the articular surfaces due to arthritis (e.g. rheumatoid arthritis, osteoarthritis) of the humero-radial and proximal radio-ulnar joints resulting in bone deterioration may cause fractures. .
Symptoms:
1. Pain on the outside of the elbow
2. Swelling in the elbow joint
3. Difficulty in bending or straightening the elbow
4. Inability or difficulty in turning the forearm (palm up to palm down or vice versa)
Non-operative treatment:
Conservative treatment is usually appropriate for Type I radial head fractures. An undisplaced fracture of radius does not require manipulation. For fractures in adults with slight displacement, an attempt is always made to reduce the fracture with manipulation. In children, closed reduction alone is often successful. After closed reduction, sling immobilization with active motion is a treatment of choice. The addition of a posterior splint for a few days is more comfortable for the patient. Initial pain control includes cryotherapy, NSAIDS, and pain relievers. Protection of the radial head from accidental bumping is achieved by elastic wrapping or loosely taping a molded thermoplast over the outer side of elbow.
Operative treatment:
Radial head fractures are common injuries which occur in about 20 percent of all acute elbow injuries.
This type of treatment is indicated for radial head fractures Type II-IV. Surgery is an option when closed manipulation has failed. There are two types of operative treatment: radial head resection and open reduction internal fixation. Open reduction internal fixation technique has shown to have better results. In this method, the fractures are internally fixed with the use of mini-plates or Herbert screws. The radial head facture is accessed through a lateral or postero-lateral approach. The fracture can be reduced by small forceps, tenacular clamps, or can be fixed with Kirschner wires. Ligaments are sutured back into place after reduction. The elbow is then fitted with a long arm cylinder cast and the elbow is kept at 90 degrees of flexion. The cast needs to be worn for 2 weeks after which it is changed to a hinged brace to allow elbow movement in the following 4 weeks period of healing.