Low Back Intervertebral Disc
Introduction
Lumbar disk disease is a frequent source of low back pain.
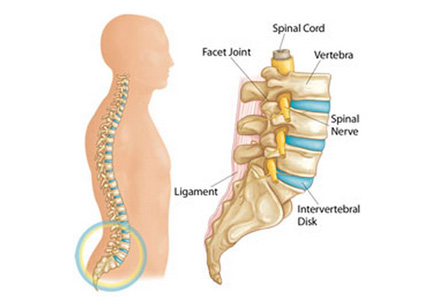
The intervertebral disks act as shock absorbers and are found between the bodies of the vertebrae. The disk consists of a central area composed of a colloidal gel, called as the nucleus pulposus, which is surrounded by a fibrous capsule known as the annulus fibrosus. This structure is held together by the anterior longitudinal ligament (which is placed anterior to the vertebral bodies) and the posterior longitudinal ligament (which is posterior to the vertebral bodies and anterior to the spinal cord). The muscles of the trunk provide additional support.
The most common site of disk herniation is the L5-S1 interspace in the lumbosacral region. This is believed to be due to the thinning of the posterior longitudinal ligament as it extends caudally.
Some problems specific to lumbar disk disease are as follows:
1. Disk bulge – Annular fibers are intact
2. Disk protrusion – Localized bulging with damage of some annular fibers.
Iran ranks among the top 10 countries in orthopedics and Iranian surgeons perform high quality orthopedic surgeries at highly affordable prices
3. Disk extrusion – Extended bulge with loss of annular fibers, but disk is intact
4. Disk sequestration – Fragment of disk comes broken off from the nucleus pulposus
Physical presentation
Nerve roots exit the spine below the intervertebral disks. Therefore, the herniation of a disk involves the nerve root below it. The patient should be observed for abnormal gait, which is suggestive of a loss of the normal rhythm. Ambulatory patients can be made to walk on their toes to test the function of S1. Observation of the patient for abnormal posture is important as it can suggest splinting or guarding from pain. Patient’s ability to dorsiflex the foot while sitting is tested for the L5 nerve root function. Sensory examination should be done corresponding to related dermatomal areas.
Palpation of the lumbar spine and lower back is not helpful in the diagnosis of disk disease, but it can rule out other causes of low back pain.
Risk factors for lumbar disk disease include the following:
1. Age
2. Activity
3. Smoking
4. Obesity
5. Vibration (eg, driving a car)
6. Sedentary lifestyle
7. Psychosocial factors
Treatment
There is limited scope for treating the lumbar disk problems by pre-hospital care. Appropriate spinal immobilization is considered if the patient has evidence of trauma. Otherwise, simple transportation in the position of comfort is usually advised.
Patient should lie in a position in which he or she is most comfortable. The goals of medical therapy are usually to reduce the pain and inflammation.
Muscle relaxants are of limited use, and clinical studies have not proven their efficacy. These medications include benzodiazepines, methocarbamol, and cyclobenzaprine. Patients should be warned that all of these drugs can cause some sedation.
Opioids provide very effective acute pain relief, but they should not be used in patients with chronic pain.
The goals of medical therapy are usually to reduce the pain and inflammation.
Salicylates, acetaminophen, and nonsteroidal anti-inflammatory drugs (NSAIDs) all have been used in the treatment of pain of lumbar disk disease, but none of these have been shown to be superior to the others. NSAIDs are used most commonly for the relief of mild to moderately severe pain. Although effects of NSAIDs in the treatment of pain are patient specific, but ibuprofen usually is the DOC for initial therapy. Other options include flurbiprofen, ketoprofen, and naproxen.
Inpatient care generally is not required, except for rare cases of intractable pain or in cases in which the social situation does not allow adequate home care. Inpatient care mostly consists of continued analgesics, physical therapy, and possible consultation with a spine specialist.