Knee Revision
Introduction
A replacement joint can sometimes wear out, become loose or develops a problem. It can be resurfaced or replaced in a joint revision operation. The orthopedic surgeon can monitor and detect any changes in the artificial joint using regular X-ray examinations. This can help to plan for revision surgery before a major problem develops.
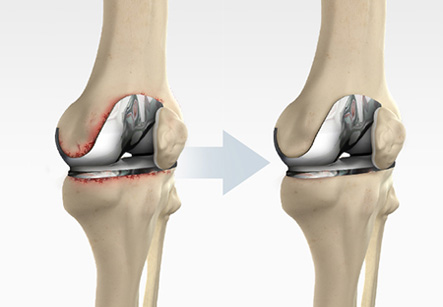
In revision knee surgery, the surgeon removes the original prosthesis, its cement, surrounding tissue and dead bone before inserting a new prosthesis. New techniques have developed for hip and knee revision surgery, which achieve better outcomes and also cause fewer complications.
Objective of knee revision surgery
1. Pain is the primary reason for performing revision. Usually the cause of pain is clear but not always. In patients without an obvious cause for knee pain, the surgery is usually not very successful if done for this purpose.
2. Plastic (polyethylene) wear- This is one of the easier revisions in which only the plastic insert is changed.
3. Instability- this means the knee is not stable and may be giving way or not feel safe while walking.
Iran ranks among the top 10 countries in orthopedics and Iranian surgeons perform high quality orthopedic surgeries at highly affordable prices
4. Loosening of either the femoral, tibial or patella component. This usually presents as pain but may be asymptomatic. For this loosening problem, the joint needs to be followed up for life as there can be changes on X-ray that indicate that the knee should be revised despite having any symptoms.
5. Infection-usually presents as pain as well as swelling or an acute fever.
6. Osteolysis (bone loss). This can occur due to loose particles being released into the knee joint which cause bone destruction.
7. Stiffness-this is usually difficult to improve with revision
The procedure
The patient is explained prior to the revision surgery what is likely to be done. However, in revision surgery the unexpected can happen and good planning can prevent most potential problems. The surgery is often more extensive than the previous surgery and the complications tend to be similar but more frequent than the first operation. This can occur as the anatomy of the muscles and tissues is not normal due to previous surgery and the scars formed may make the exploration of structures difficult.
The surgery can vary from a simple liner exchange to changing one or all of the components. Extra bone may need to be used to make up for any bone loss.
1. The surgeon makes an incision in front of the knee exposing the knee joint.
2. The knee cap and its ligament may be moved or retracted to make room for the operation.
3. The surgeon usually removes the old femoral component.
4. The femur is then prepared to accept the new component. Sometimes the damaged bone needs to be removed.
5. After this, the femoral component is fixed in place. Sometimes extra bone or a metal wedge may be used to make up for the lost bone.
6. Occasionally cement may be used depending on surgeons’ preference.
7. The surgeon then focuses on the tibia to remove the tibial component along with the old plastic liner. The damaged bone is excised.
8. The tibia is then prepared to take the new tibial component. According to surgeon’s preference, the lost bone is then replaced either by a metal wedge or bone graft.
9. The tibial component is secured to the end of the bone by using bone cement or screws depending on a number of factors and on surgeon’s choice.
10. A new plastic liner is placed on the tibial component. Occasionally, the knee cap may also be prepared to receive a plastic component.
11. The femoral and the tibial component are fixed in place to form the new knee joint. After completion of the procedure, the muscles and tendons are approximated. Drains are usually inserted to drain excessive blood.
Complications from Revision Knee Surgery May Include:
1. Infection (in only a few cases).
2. Loosening of the new prosthesis- The likelihood of this complication is much greater if patient is overweight and does not use crutches during the first few months.
3. Dislocation of joint. This is twice as common as for a primary procedure.
4. One leg can become shorter than the other.
5. Bone loss in the joint which may need grafting