Knee Replacement Surgery
Introduction
The knees are the joints that bear the weight of the body. Chronic arthritis, injuries or severe infections can lead to painful stiff knees that can prevent one from getting around even for the daily activities. It is when all other medications and therapies fail that patient may consider a Total Knee Replacement or TKR.
The knee joint is essentially made up of the thigh bone or femur that sits on the upper part of the shin bone or tibia. There is the knee cap or patella over the joint to assist in movement and provide stability to the joint. The joint space has cartilages to cushion and assist the smooth movement of the knee.
Iran ranks among the top 10 countries in orthopedics and Iranian surgeons perform high quality orthopedic surgeries at highly affordable prices
Surgery Procedure
Before the operation the surgeon will need to get the knee X rayed for detailed diagnosis.
Knee replacement operation is usually performed under general anesthesia wherein patient will be rendered unconscious during the operative procedure. This operation can also be done under spinal or epidural anesthesia wherein the anesthetic drug is injected between the vertebrae and it helps to numb all sensations of the legs during the operation.
A cuff like tourniquet is placed on the thighs just before the incision. When inflated this aids in reducing the blood flow to the operative site and reduces the risk of bleeding. If patient is at risk of developing blood clots or thromboembolism, then the tourniquet may not be applied.
The damaged parts of the joint including the lower part of the femur, upper part of the tibia are removed or sawed off.
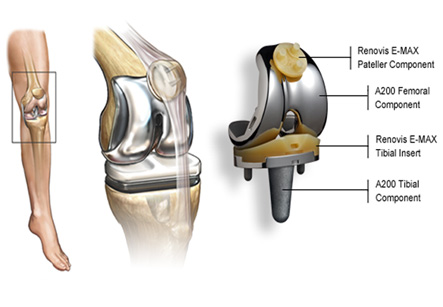
There are basically two approaches to a TKR. One is the classical method and another is the newly developed Minimally Invasive Surgery (MIS). In classical TKR an eight to twelve inch incision is made in the front or side of the knee. The muscles are cut open and the joint cavity is exposed. The damaged parts of the joint including the lower part of the femur, upper part of the tibia are removed or sawed off. The prosthesis or the artificial joint is a metallic or plastic replica of the lower part of the thigh bone and upper part of the tibia. The new implants are sealed on the sawed off edges with the help of bone cement. Some implants are uncemented. These can be set over the edges of the sawed off bones in a press fit system. Prosthetic cartilage is placed between the prosthetic ends of the femur and tibia.
Minimally Invasive Surgery as the name suggests involves a smaller incision of three to five inches. Here the surgeon works the implant through a smaller opening. This leads to less pain and more rapid recovery. The tourniquet is removed or deflated before the incision is closed in order to check for any bleeding points. The surrounding muscles and ligaments are sewn back together and these provide stability to the joint and assist it in movement. The skin incision is closed with a drainage pipe to drain the excess fluids and the wound is bandaged. The knee is cast in a splint to aid recovery. The pulses of the feet are checked before removing the patient from the operative table to assess that the blood flow to the feet is intact after the cast.
Recuperation and post operative complications
Patient will be removed to Highly Dependency ward from the operation theatre wherein they will be given intravenous fluids, antibiotics and pain relieving medications. After 24 hours patient will be transferred to the hospital bed from which they will be discharged in a week or two.
From the initial recovery period movement of the knee is encouraged. This is done under the guidance of a physiotherapist. Patient may be allowed knee exercises under supervision or the use of Continuous Passive Motion (CPM) machine. Early mobilization of the joint aids in rapid recovery and also prevents formations of blood clots that can lead to life threatening condition of thromboembolism where this clots can move up to the lungs or block the blood flow to the heart or brain. Blood thinning medications are also prescribed if they are prone to develop blood clots and these may be continued even after the discharge. On discharge patient may need crutches, walker or a cane to walk. After around six to eight weeks they will be able to walk with minimal assistance.
Risk of infection, pain, blood clots, nerve damage and fractures of the bones during or after the operation are associated with TKR. Benefits of this operation are remarkable in terms of freedom from pain, improved range of movement of the knees, improved sleep and better quality of living.
The non-surgical alternatives to Total Knee Replacement TKR include pain and anti-inflammatory medications, moist heat and physical therapy. Weight loss and injections of cortisone into the knee joint can also ease painful arthritic knees to a large extent. Walking with the aid of crutches, cane or special braces are other alternatives to TKR. Short operative procedures like replacement or transplant of cartilage can also relieve pain and improve movement.