Femoral Shaft Fracture
Introduction
The femur or thigh bone is the largest and strongest bone of the body and has a good blood supply. It is surrounded by strong thigh muscles. Because of these factors, the shaft requires a considerable amount of force to fracture. Once a fracture occurs, the same protective musculature causes complications like displacement, which commonly occurs with femoral shaft fractures.
Causes of fracture shaft femur:
1. Severe trauma
2. Pathological lytic lesions
3. Metastasis from distant primary cancer
4. Paget’s disease
5. Bone cysts
6. Osteoporosis
Iran ranks among the top 10 countries in orthopedics and Iranian surgeons perform high quality orthopedic surgeries at highly affordable prices
Patho-anatomy of fracture:
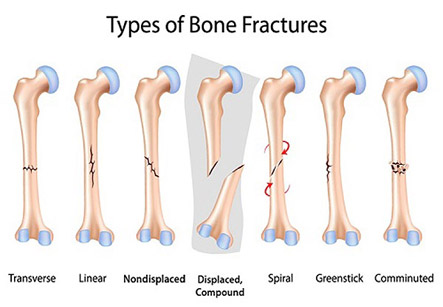
The fracture can occur anywhere in the upper, middle and lower-thirds of the shaft of femur. It can be of mainly of three types:
Type I – Spiral or transverse (most common)
Type II – Comminuted causing fragments of bone
Type III – Open. In this the bone fragments can be seen on the surface.
Clinical features:
1. Pain
2. Swelling
3. Deformity
4. Abnormal mobility due to fracture
Diagnosis:
Brief medical history and physical examination are done. This can lead to the cause of non-traumatic fracture in some cases. No specific lab tests are needed in an emergency case.
The fracture can occur anywhere in the upper, middle and lower-thirds of the shaft of femur.
In a patient with a large, expanding hematoma in the thigh, only hematocrit and blood typing and cross-matching is done in case a blood transfusion becomes necessary.
For patients who require open reduction and internal fixation of fracture preoperative tests such as chest radiography and ECG needs to be done.
Imaging Studies:
As in case of any long bone fracture, antero-posterior (AP) and lateral X-ray views of the femur above and below the fracture level are necessary. In case if the vascular injury is suspected, femoral angiography is recommended.
Treatment:
There can be two methods of treatment.
A. Conservative methods:
1. Traction: Traction with or without splinting is useful in treatment of fracture of shaft femur. Skin traction is sufficient in children but skeletal traction (in which the traction is supported by pins piercing through the bone) through an upper tibial Steinmann pin is required in adults. Thomas splint is needed in this treatment.
2. Hip spica: It is the name of plaster cast used in fracture shaft femur which incorporates both limb and part of a trunk. It is of two types- single and one and half spica. This is used for immobilization in children and young adults after the fracture becomes sticky.
B. Operative methods:
1. Closed reduction and internal fixation-
The internal fixation may be an intramedullary nailing or plating. These are some of the common used methods of internal fixation.
• Closed intra-medullary nailing:
A steel nail is introduces in the femoral medullary canal through the greater trochanter under intra-operative fluoroscopic guidance. The fracture site is not exposed; therefore better results are obtained compared to conventional open nailing.
• Inter locking nailing:
In this method, nail is introduced in the same way as the intramedullary nailing. But this nail has holes at both the ends for locking the bone at one or both the ends by screws. The special screws pass from one cortex to the other cortex through the inside of the nail.
• Kuntscher’scloverleaf intra-medullary nailing (k- nail):
This method is used in transverse or a short spiral fracture at the junction of the upper and middle thirds of the femur. It is not preferred for fragmented fractures, fractures in the distal third of shaft and in open fractures.
• Plating
This is preferred when the medullary canal is wide, so K-nail cannot provide the required grip. Plating is also done in case of comminuted fractures.
2. Open reduction:
This therapy requires reduction by exposing the fracture site followed by fixation to maintain the alignment of fractured segments. Options include external fixation or internal fixation. Internal fixation is with intramedullary devices (flexible rods, rigid retrograde or ante-grade rods) or extra-medullary plates and cortical screws.
Complications:
Early complications:
1. Injury to femoral artery
2. Sciatic nerve injury
3. Shock
4. Fat embolism
5. Infection
Late complications:
1. Non-union
2. Mal-union
3. Delayed union
Physiotherapy:
Physiotherapy after a few weeks of surgery helps in:
1. Pain relief
2. Restores range of motion of joint
3. Muscle strengthening
4. Improvement of gait
5. Prevention of complications
6. Restoration of daily activities