Anterior Cruciate Ligament Reconstruction
Introduction
Ligaments are tough bands of tissue which connect the ends of two bones together. The ACL is a 3 to 4 cm long fibrous band located in the centre of the knee joint. It runs from the backside of the femur (thighbone) to connect to the front of the tibia or shinbone.
The ACL runs through a special notch in the femur called as the intercondylar notch. It also attaches to a special area of the tibia called the tibial spine.
The ACL controls and limits the forward movement of the under the femur. If the tibia moves too far, the ACL tends to rupture. The ACL is also the first ligament that becomes tight when the knee becomes straight. It helps stabilize the knee joint when performing twisting actions. This ligament is usually not required for normal daily living activities. However, it is essential in controlling the rotation forces developed during side stepping, pivoting and landing from a jump.
The ACL passes through the joint and is surrounded by joint fluid. When ACL is injured, the bleeding fills the joint, causing pain and swelling. Some patients frequently hear or feel a snap, or crack accompanied by pain. Swelling commonly occurs within an hour. Sometimes, joint dislocates and reduces with a clunk. The injury causes a sense of instability and insecurity. The blood clot does not form in the joint cavity due to its unique synovial fluid. Therefore, scar tissue does not form. The result is that the ACL rarely heals in continuity.
Iran ranks among the top 10 countries in orthopedics and Iranian surgeons perform high quality orthopedic surgeries at highly affordable prices
The ACL is commonly injured whilst playing running ball sports or skiing. Whilst playing ball sports, landing from a jump or side step maneuver cause the knee to give way. When skiing, rupture may occur at low or high speeds.
The knee usually has a tendency to swell in the first 6 weeks.
Initial treatment of any knee ligament injury consists of ice packs, compression bandages and crutches. Weight bearing is very difficult for several days. The swelling starts to settle after seven to ten days the walking is possible with the joint returning to full range of motion. The knee joint becomes almost normal by about four weeks following the injury. The further episodes of instability can result in multiple injuries to the cartilages and the joint surfaces. Damage to these structures can lead to early-onset osteoarthritis.
Conservative Treatment
Conservative treatment is by physical therapy is done whether surgery is planned or not. The conservative approach is aimed at reducing swelling, restoring the range of motion of the knee joint and also to restore full muscle power. Proprioceptive training is given to the patient to develop the necessary protective reflexes required to protect the joint from injuries during normal daily living activities. As the cruciate ligament controls the joint during changes of direction, it is important to play only the sports involving straight line activity only. Social (non-competitive) sport may still be possible without instability as long as there is no sudden change of direction.
Surgical ACL reconstruction
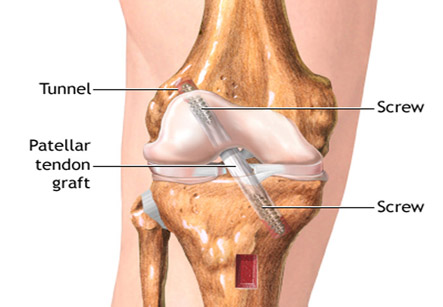
The ACL tear cannot be sutured back in place exactly as it was earlier. In the reconstruction surgery, a graft is harvested to use to rebuild the torn ligament. The graft is taken from 2 of the hamstring tendons, but sometimes other suitable graft choices can be used. The choice will be discussed with the patient prior to the operation. The remnants of the torn ACL are removed with keyhole or small incision. Tunnels are made in the tibia (shin bone) and femur (thigh bone) to allow this graft to be positioned across the knee joint. The new reconstructed ligament is then fixed at both the ends to secure it in place.
Post-operative care
The patient wakes up in recovery with bandages around the knee joint. There may be a small drain coming from the knee to drain any excess bleeding and also to reduce the swelling. Pain-relievers are given if required. It is safe to move the knee, but patient is advised to keep the knee straight while resting. Weight-bearing on the knee is safe, but it is more comfortable to start walking with some elbow crutches for first few days. By 1-2 weeks the patient can walk normally. Driving is normally safe after this stage.
The knee usually has a tendency to swell in the first 6 weeks. Ice compresses are important to apply on the knee between exercises and when resting to keep it elevated.
Some exercises are given to help in rehabilitation of the knee.