Ventricular Reduction
Introduction
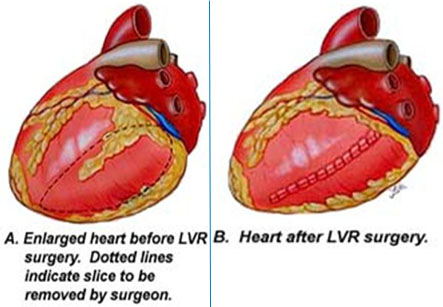
Left ventricular reduction surgery is designed to reduce the size of an enlarged heart instead of a performing heart bypass in some cases.
Recently, the cardiac surgeons have begun performing a new surgical procedure, called as left ventricular reduction. This is being tried at many Heart Institutes on selected patients with enlarged, failing hearts, in a condition known as congestive heart failure. This operation may be an effective alternative to heart transplantation for some patients. This procedure involves removing a slice of muscle from the enlarged heart and sewing the heart back together. By reduction of its size, the heart can pump more efficiently and vigorously.
Congestive heart failure occurs when an enlarged, weakened heart cannot work efficiently and causes a build-up of fluids in the body due to a reduction in blood flow. Blood returning to the heart congests the veins and forces fluid into surrounding tissues, most often the feet and legs. As a result, the feet, legs and ankles begin to swell under the increased fluid volume, and this condition is known as edema. This edema can spread to other parts of the body, including vital organs. If the fluid accumulation occurs in the lungs, it can cause a life-threatening situation. The reduction in blood flow is caused by the enlargement of the heart, as an enlarged heart does not have the capacity to pump as efficiently as a normal heart.
Iran is among the top 10 countries in treating cardiovascular diseases, while it ranks first in the Middle East
Heart assist devices can help patients until left ventricular reduction surgery can be performed.
Heart assist devices are used by the surgeons during the waiting period for the left ventricular reduction procedure. By implanting the assist device, the heart can get some rest and the damaged heart cells may return to normal. The assist device can then be removed, and a left ventricular reduction can be performed. The initial results of this procedure are promising.
The left ventricular volume reduction surgery was originally proposed by Dr Batista to reduce the dimensions of the dilated left ventricle by excising a sizable amount of the ventricular free wall. The mechanism of cardiac improvement totally depends on La Place’s law, therefore left ventricular wall tension is decreased by reducing its diameter. This results in an increase in ejection fraction. However, some questions regarding the diastolic function, preoperative judgement of left ventricular wall characteristics and late re-dilatation of the left ventricle, are still unanswered. The operation was originally performed using normothermic cardiopulmonary bypass on the beating heart.
The procedure
The procedure is performed through a median sternotomy, followed by standard cannulation of the ascending aorta and selective bi-cavalcannulation.
Originally, the operation was carried out on the beating heart. An incision is then made at the apex of the dilated left ventricle. This is followed by anterior and posterior ventriculectomy incisions extended toward the atrioventricular groove and brought together 1–2 cm prior to reaching it.
The posterior ventriculectomy may be extended beyond the posterior medial papillary muscle in case a larger reduction is planned with associated mitral valve replacement.
The procedure is performed through a median sternotomy, followed by standard cannulation of the ascending aorta and selective bi-cavalcannulation.
After this, the surgeon closes the ventriculectomy using a continuous 2-0 monofilament full-thickness suture, followed by 3-0 monofilament hemostatic suture.
This suturing will determine the new shape of the LV with reduction of left ventricular volume and size.
Several variations of the technique have been developed depending on the need of appropriate myocardial protection during surgery. The suture line may be reinforced to prevent catastrophic bleeding. The variations also depend on the presence of associated cardiac pathologies such as mitral and/or tricuspid valve regurgitation.
Although the original technique was to perform surgery with normothermic cardiopulmonary bypass on the beating heart, some surgeons prefer to induce cardioplegic arrest for 3 reasons:
1. to optimise myocardial protection, particularly in presence of coronary artery disease
2. to enhance manual handling, improve assessment of the area to be resected, and facilitate valve repair if needed
3. to facilitate the achievement of a more haemostatic suture line.
Reinforcement of the suture line to prevent catastrophic bleeding may further be achieved by buttressing of the suture line with pericardium or Teflon felts, and alternatively by using biological glue.
In case of associated significant mitral regurgitation, this is also corrected by an edge-to-edge repair performed directly from the ventricular side.
In case of associated significant tricuspid valve regurgitation, it is corrected by standard repair techniques