Cardiopulmonary Bypass
Introduction
The cardiothoracic surgeon requires a bloodless, motionless field for work to repair most of the cardiac defects. For this purpose, the motion of the heart and lungs must be stopped.
This is not as simple as it appears to be. For this, there needs to be a means for blood to circulate throughout the body to deliver the oxygen and nutrients necessary for life, while the heart and lungs are stopped. This is made possible through a process known as cardiopulmonary bypass (CPB).
Although the cardiopulmonary bypass originated in the 19th century, the field has developed rapidly in the last 50 years. The first attempt to use a heart-lung machine for total cardiopulmonary bypass was carried out in 1951. Since that time, this technique has become a standard, widely used, low-risk procedure.
Procedure
Iran is among the top 10 countries in treating cardiovascular diseases, while it ranks first in the Middle East
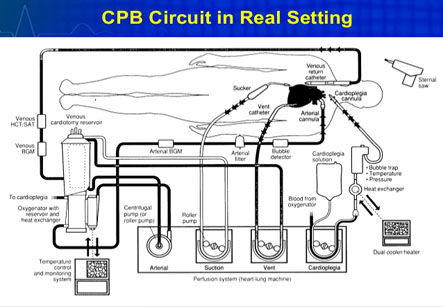
The patient’s blood which is diverted from the body flows in tubing made up of clear polyvinyl chloride (PVC). Large bore catheters (called as cannula) are placed in the right side of the heart, which allow the desaturated blood from the body to enter the cardiopulmonary bypass circuit.
The PVC tubing runs through a mechanical pump that can be regulated according to required cardiac output for a particular patient. The cardiac output depends on the surface area of the body. Thus, a 5-year-old child has a much smaller cardiac output than an adult. Therefore, the pump must run at a higher rate for the adult patient than the child. More PVC tubing delivers blood from the mechanical pump to another gas exchange device called as an oxygenator, or artificial lung.
This oxygenator performs the same job as the lungs: oxygenation of the blood as well as removal of carbon dioxide. The re-oxygenated blood returns again to the body via another cannula placed in the aorta. Thus, the cardiopulmonary bypass permits the patients’ blood to bypass the heart and lungs. As a result, the desired bloodless, motionless operative field can be achieved without interrupting a constant supply of oxygen and nutrient-rich blood to all the other organs of the body.
The assembly of the mechanical pump, oxygenator, cannula and PVC tubing is often referred to as the heart-lung machine or simply “the pump.”
When the circulation of a patient is being supported by the heart-lung machine, the patient is said to be “on bypass” or “on the pump.” Whereas, when a patient is taken off of this support, it is termed “off bypass” or “off the pump.” This terminology is very important for the cardiac surgeon during the actual surgical procedure.
However, it should be kept in mind that there are certain adverse effects which can occur while the circulation of the body is taken over artificially. Cardiopulmonary bypass have a wide range of effects on the body. All organ systems are affected by cardiopulmonary bypass including the heart, lungs, brain and kidneys.
These effects can range from mild to severe depending on the medical condition of the patient before surgery, the length of time that a patient is supported by cardiopulmonary bypass and the complexity of the operation being performed.
The function of the heart may be compromised to some degree after bypass surgery. Some patients can develop mild neurological changes after bypass surgery. There is a possibility of stroke or seizures during or after bypass, but it is relatively rare.
There may also be kidney damage resulting from decreased urinary output to complete renal failure. Areas of the lung may also fail to fully expand after bypass. This condition is known as atelectasis.
The patients’ blood is in contact with the foreign surfaces (PVC tubing) that are parts of the heart-lung machine. This can lead to a reaction by the patient’s body involving a generalized inflammatory response, swelling of different body parts, fever and abnormal blood tests.
The risk of serious complications as a result of cardiopulmonary support depends upon the age of the patient, general condition and the complexity of the surgery to be performed.
Research has shown that this response can be potentially damaging to certain tissues in the body. This inflammatory response can be minimized with preoperative and intraoperative treatment with steroids and sometimes by the use of medicine called as aprotinin.
Extra volume of fluid is needed to fill the cardiopulmonary bypass circuit, which can dilute the patients’ blood volume. This may require transfusion of blood products to the patient while on cardiopulmonary bypass. Blood clotting abnormalities can also occur during the post-operative period.
The risk of serious complications as a result of cardiopulmonary support depends upon the age of the patient, general condition and the complexity of the surgery to be performed.