Balloon Septostomy
Introduction
Balloon atrial septostomy is a procedure involving creation of an atrial septal defect without thoracotomy or anesthesia. This can be performed rapidly in any cardiac catheterization laboratory. A variety of catheters can be used for balloon atrial septostomy. The most commonly used catheter in modern cardiology is 5F Miller balloon atrial septostomy catheter which needs a 7F to 8F introducer. The dual lumen Z-5 atrio-septostomy catheter 13, comes in 4F or 5F sizes, depending on the balloon diameter and requires a 5 or 6F introducer, respectively. The Z-5 catheter requires to be advanced over a guidewire, as opposed to the Miller catheter.
The technique
This procedure can be performed under sedation or general anaesthesia. The access to the heart is achieved via the femoral or the umbilical vein. The femoral vein is punctured and a 4F or 5F introducer is placed in the vessel and then exchanged for a 7F or 8F introducer, when the Miller catheter is used. After this, the balloon catheter is advanced into the right atrium. The foramen ovale is crossed and the catheter is positioned in the left atrium. Correct positioning is critical and it is guided by a biplane fluoroscopy or two-dimensional echocardiography. It is recommended to position the catheter tip in the orifice of the left upper pulmonary vein, to confirm its left atrial location.
Iran is among the top 10 countries in treating cardiovascular diseases, while it ranks first in the Middle East
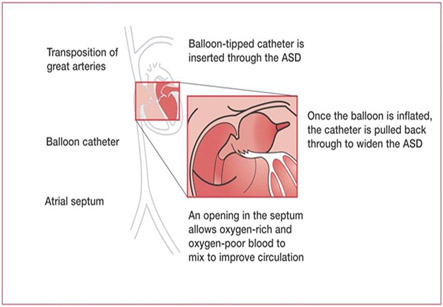
The balloon is inflated rapidly with 3-4 ml of dilute radiopaque solution, locked, and then sharply withdrawn into the right atrium. The catheter is then advanced into the body of the right atrium, so as not to obstruct inferior caval return, and then deflated rapidly. This process is repeated two to three times. The size of the newly created inter-atrial communication can be measured directly by echocardiography at the table. The efficacy of the shunt is immediately obvious, from the rise in arterial oxygen saturation.
This procedure can be performed under sedation or general anesthesia.
Umbilical venous approach: The umbilical cord is cut transversely very near to the skin. The vein inside is identified, and the catheter is directly inserted into the vessel with a forceps. The progress of the catheter through the ductusvenosusis monitored either by fluroscopy or by cross sectional echocardiography. After reaching the right atrium, the procedure done is similar to femoral vein approach. Sometimes it can be difficult to pass the catheter into the inferior vena cava due to closure or narrowing of the ductusvenosus. In this case a guidewire and 4F catheter can be introduced into the umbilical vein, and then advanced into the right atrium. After this, the septostomy catheter is introduced with the help of 7F or 8F sheath. It is important to remember to withdraw the sheath well into the ducutsvenosus before performing the septostomy. With the Z-5 atrioseptostomy catheter, it is easy to position the guidewire in the left upper pulmonary vein. The balloon catheter is advanced over the wire into the left atrium like in conventional septostomy.
Although it is a safe procedure, various complications have been reported in various patients. They can include:
1. Rhythm disturbances such as premature ectopic beats, supraventricular tachycardia, atrial flutter and fibrillation, partial or complete heart block and ventricular arrhythmias
2. Perforation of the heart
3. Dislodging of balloon fragment in blood
4. Injury to the atrioventricular valves, systemic or pulmonary veins
5. Failure of balloon deflation.
In practice, the complications associated with the procedure are unusual at the present day.
Indications:
Common indications for balloon atrial septostomy are:
1. Transposition of the great arteries with or without associated cardiac defects. The benefit of surgery may be limited if the systemic saturation can be adequately maintained with prostaglandin E infusion alone.
2. Tricuspid valve atresia
3. Pulmonary atresia with intact ventricular septum
4. Total anomalous pulmonary venous connection with restrictive ASD
5. Hypoplastic left heart syndrome for emergency relief of the gradient across the septumin neonates. Balloon atrial septostomy is an effective treatment for infants less than six weeks. It is, however, not suitable for children older than 1-2 months.