Aortic Valve Replacement
Introduction
Aortic valve replacement, also known as AVR, is a procedure in cardiac surgery which replaces a patient’s failing aortic valve with an alternate healthy valve. This is generally an open heart surgery. In some cases, a percutaneous approach is used but there is more risk of stroke in this method.
Indications:
There are several heart valve disorders in which the patient needs to undergo AVR. However, the two most common diseases for which aortic valve replacement is required are:
Aortic Stenosis: It is the name given to a condition of narrowing of the aortic valve. The blood flow through the valve is constricted. This can happen as a result of degeneration of leaflets of the valve or calcification.
The patient requires staying for at least 12 to 36 hours in the intensive care unit after the aortic valve replacement.
Iran is among the top 10 countries in treating cardiovascular diseases, while it ranks first in the Middle East
Aortic Regurgitation: In this case, the leaflets of the valve become loose or floppy causing blood to leak back into the left ventricle. It is also called as aortic insufficiency as the valve is insufficient to maintain the blood flow in one direction.
Less commonly, Aortic valve disease can result from a congenital defect. Or, it can be caused by a serious bacterial infection of the valves. Calcified aortic valves need replacement.
Types of heart valves
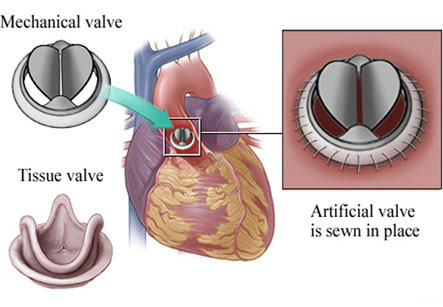
There are two basic types of artificial heart valves: mechanical valves and biological valves.
1. Biological valves: These valves are made from animal tissue like animal heart valve tissue or animal pericardial tissue. Generally, cattle or pig tissues are used. The tissue is pre-treated to prevent rejection and calcification after replacement. In some cases, a homograft or a human aortic valve can also be implanted. Homograft valves are donated by willing patients and recovered after the death. The homograft is as durable as porcine or bovine tissues.
2. Mechanical valves: Mechanical valves are long lasting and tested to endure for patient’s entire lifetime, giving a permanent solution. One surgery can improve patient’s life. But, there is increased risk of formation of blood clots by mechanical valves. Therefore, life-long treatment with anticoagulants is needed in these patients who have a side effect of making the patient vulnerable to bleeding.
Valve selection:
Which type of valve should be used depends on an important factor- the patient age. Life of the Tissue valves depends on the flow demand across the replaced valve. It wears out faster with increased flow demands. So they are used in younger individuals. Tissue valves last for 10–15 years in elderly patients, as they are less active and need less flow across the valve. After wearing of tissue valves, a repeat valve replacement surgery is needed. Therefore, younger individuals are advised to get a mechanical aortic valve in their heart.
Surgical Procedure:
1. Under general anesthesia, an incision is made by cutting the sternum, called as median sternotomy.
2. After opening the pericardium, the patient is put on a cardiopulmonary bypass machine, also known as the artificial heart-lung machine. This machine maintains the task of breathing and pumping the blood in the body while the surgeon replaces the heart valve.
3. A cross-clamp is applied after taking an incision in the aorta. Diseased aortic valve is then removed and is replaced by a new mechanical or tissue valve.
4. After this, the aorta is closed and patient is taken off the heart-lung machine.
5. An ultrasound of the heart done through the esophagus also called as trans-esophageal echocardiogram is used to check the proper functioning of the new valve.
6. Pacing wires are put inside the surgical area; so that the heart can be paced from outside if any complications arise after surgery.
7. Small drainage tubes are then inserted to drain fluids or blood coming from the chest and pericardium after the surgery. The drains are removed within 36 hours and the pacing wires are left in place till the patient is discharged from the hospital.
Ross procedure:
In this procedure, the aortic valve is removed and it is replaced by the patient’s own pulmonary valve. Then, the patient’s pulmonary valve is replaced in turn by a pulmonary valve taken from a cadaver or pulmonary homograft. This procedure is usually performed in children as the patient’s own pulmonary valve-which is now in place of aortic valve-also grows with the child.
Hospital stay and recovery time:
The patient requires staying for at least 12 to 36 hours in the intensive care unit after the aortic valve replacement. The patient can go home after about four days, unless any complications arise.
Total recovery from the surgery takes about three months, if the patient is in good health. Patients are advised to avoid lifting heavy weights for 4–6 months after surgery to avoid damage to the sternum or the breast bone.
Surgical outcome and risks:
The risk of death or serious complications from aortic valve replacement is between 1-3%. This depends on the health and age of the patient, as well as the skill of the cardiac surgeon. Older patients and patients with other serious diseases are sometimes ineligible for surgery because of raised risks.