Salpingography
Introduction
A salpingography is an important diagnostic test for evaluating female fertility potential. This is a radiological procedure usually done in the radiology department of a hospital or outpatient setup having radiology facility.
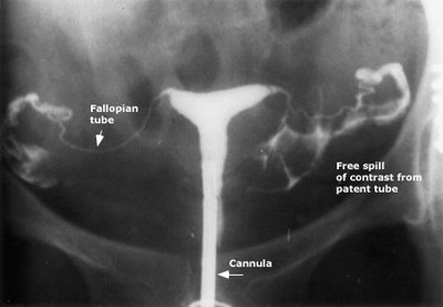
In this procedure, a radio-opaque contrast or dye is injected into the uterine cavity through the vagina and cervix. The uterine cavity fills with dye and if the fallopian tubes are open, dye fills the tubes and spills into the abdominal cavity.
This can evaluate the tubal factor of infertility. It confirms whether the fallopian tubes are open or blocked and also finds the site of blockage in the tube. The blockage can be at the junction of the tube and uterus (called as proximal) or at the abdominal end of the tube (distal).
If the tubal factor of infertility is found to be present, it can be treated early and couples can conceive in result.
Partial blockage of fallopian tubes, defects in the tube or pelvic scar tissue in the abdominal cavity near the tube can be diagnosed by this examination.
About 85-90% of women will have at least one tube opened and about 60% will remain open at 6 months if rechecked. We have all the information you need about public and private clinics and hospitals that provide gynaecological treatment in Iran
Procedure:
1. The salpingography study is usually done in the radiology department or operation room having X-ray facility of a hospital so there is additional time for the woman to register at the facility and fill out a questionnaire and answer questions regarding allergies to medication etc.
2. The position for the procedure is lying on the back on an examination table with feet raised and supported by foot rests or foot stirrups.
3. An instrument with smooth, curved blades known as speculum is inserted in the vagina to visualize the opening of uterus known as cervix.
4. For injecting the dye, a soft, thin catheter may be passed through the cervical opening into the uterine cavity. Otherwise, an instrument called as a tenaculum is placed on the cervix and then a narrow metal cannula is passed into the cervical opening.
5. This catheter or cannula is used for injecting the contrast dye into the uterine cavity.
6. An x-ray shoot is taken as the uterine cavity fills with the dye and then additional contrast is injected to fill the tubes and to spill into the abdominal cavity. More x-ray pictures are taken of this filling and spilling.
7. After confirmation of tubes spilling the dye (this means tubes are patent.
8. Sometimes the dye will not flow into the tube(s) because of an obstruction or “spasm” of the muscle around the opening of the tube. With an HSG alone, it is impossible to distinguish an obstruction from spasm (which is of no importance). Furthermore, if a true obstruction exists, there is no way to bypass it by HCG alone.
9. With selective salpingography, a smaller diameter, flexible catheter is run inside the HSG catheter. Under the guidance of live x-ray, this catheter can be directed right into the opening of the fallopian tube. Once this is done, dye can be introduced directly into the fallopian tube.
10. With this technique, it is possible to diagnose a normal, patent, fallopian tube whose opening may be in spasm. Fallopian tubes with an actual obstruction require higher pressures foe opening which can be achieved with selective salpingography. However, it should be noted that this procedure may not always be successful in opening an obstructed tube.
Steps in elective salpingography:
First a 5.5 french 2 mm catheter is guided into the corner (cornua) of the uterus. An attempt is made to pass dye. If this is successful, the woman probably had spasm of the tube and this also means that the tubes were never really blocked. That is one of the weaknesses of regular HSG. If patient is mentally scared or in pain, the tubes go into spasm and appear blocked even if there is no obstruction.
If they are still not open, a 1mm catheter is passed into a tube and then a .018mm guide wire is moved into the fallopian tube. This dislodges any debris in the tube. The other catheters are then passed over the wire. Sometimes a balloon catheter is needed to dilate the tubes. Once the catheter is in the tubes, the selective HSG is repeated. If the distal end of the tube is still normal, the chances of conceiving are usually good.
About 85-90% of women will have at least one tube opened and about 60% will remain open at 6 months if rechecked. 30-40% women undergoing this procedure usually conceive.
Complications
Complications associated with a salpingography include:
1. An allergic reaction to the contrast which is uncommon. This causes usually a rash, but rarely can be more serious.
2. Pelvic infection
3. Perforation of uterus is possible, but this is very rare.