Superovulation
Introduction
Superovulation therapy is a treatment for infertility which involves stimulation of ovaries using medications called as gonadotropins. Gonadotropins are hormonal fertility medications given by injection. They contain follicle-stimulating hormone (FSH), which is produced naturally by the pituitary gland. This is given alone or combined with luteinizing hormone (LH) (this is also produced bythe pituitary gland). A related medication is a hormone called as human chorionic gonadotropin (hCG). HCG has a similar structure to LH and has a function of simulating the natural LH surge that causes ovulation at midcycle.
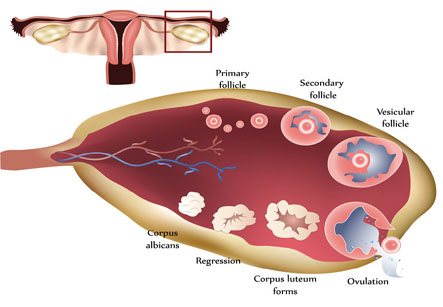
Gonadotropins are used to stimulate the growth of ovarian follicles in the ovary. Follicles are individual sacs of fluid which contain developing egg or oocyte. These drugs are used to induce ovulation in women who do not ovulate. Also, they can be used to induce development and ovulation of multiple follicles in women who need to undergo assisted reproductive therapies like superovulation and intrauterine insemination or in vitro fertilization (IVF).
Iran ranks first in the region in terms of infertility treatment studies
Indications for Superovulation:
• Unexplained or unknown cause of infertility
• Infrequent or absence of ovulation (e.g. PCOS)
• Mild male factor infertility
Procedure:
A Superovulation /IUI cycle will involve the following steps:
1) To schedule the treatment cycle, the natural menstrual cycle needs to be suppressed. This purpose can be served by a short course of birth control pills.
2) Stimulation of the ovaries with injectable hormones – to stimulate the growth of ovarian follicles (usually 2 to 4), FSH injections are given daily. The woman may be taught to give these injections to herself at home. They are taken daily for about 10-14 days, starting on day 1-3 of menstrual cycle.
3) Monitoring of treatment with transvaginal ultrasound and blood tests- this is done to determine how many eggs are developing, and when the eggs are mature and ready to ovulate.
4) Triggering of ovulation- injection of hCG is given which mimics the body’s LH surge in a natural cycle. The hCG causes final maturation of the egg(s) and also release of the egg(s) after about 36-40 hours. The timing of this injection is very important as it is necessary to accurately match the time of insemination with ovulation.
5) Timed intrauterine insemination (IUI)- on the day of ovulation, husband’s or donor’s sperm sample is provided. The sample is washed, prepared, and then placed into the uterus through the cervix with the help of a small, flexible catheter. This is a simple procedure with minimal discomfort.
6) Pregnancy testing- Following the IUI, progesterone supplementation is given. This is continued until the pregnancy test, which is done 2 weeks after the IUI. If the woman is pregnant, progesterone is continued during the first trimester.
Monitoring:
Careful monitoring of patients is required during the superovulation therapy tominimize the risk of side effects. These side effects include:
1. Medication side effects:
• Heaviness or bloating in the pelvis
• Mood changes
• Headaches
• Breast tenderness
2. Ovarian Hyperstimulation Syndrome (OHSS):
OHSS is characterized by enlarged ovaries and fluid accumulation in the abdomen after ovulation or egg retrieval. In severe cases, hospitalization is required for monitoring.
3. Multiple pregnancy:
Women conceiving with SO have a 20-25% chance of having a multiple pregnancy, the vast majority of which are twins. Triplets or higher order pregnancies can occur, but are much less frequent.
4. Ectopic pregnancy:
Ectopic pregnancies develop outside the usual location in the uterus, usually in the fallopian tube. In superovulation cycles the possibility of this event may be increased. Ectopic pregnancies can be treated with medications or surgery.
5. Birth defects and pregnancy complications:
Pregnancy-associated hypertensionand abruption of the placenta may be increased.
6. Gonadotropins and the risk of ovarian cancer:
Although early studies suggested that the risk of ovarian cancer might be increased in women exposed to this therapy, more recent studies have not shown any such relationship.
If there are some problems in this process, there are two ways to handle the situation:
1. Cycle cancellation
Each woman responds in her own way to gonadotropin medication. Sometimes the response is too fast or too strong. In such cases, the physician supervising the cycle may advice to stop the medications to avoid the risk of complications such as OHSS or multiple pregnancies. Medication dosages and protocols are reviewed and modified. This helps in reducing the risks and improving the response at the next attempt. Canceling a cycle is a rare event.
2. Conversion of a Superovulation cycle to IVF
In case of expected risk of multiple pregnancies, the cycle can be converted to IVF. This involves removing the mature eggs from the ovaries and fertilizing them in the lab. 2 or 3 embryos thus formed are replaced back into the uterus. However, the IVF conversion is more expensive if a couple decides to go ahead with it.